Product Details
| Species Reactivity |
Human (Homo sapiens) |
| UniProt |
N/A |
| Abbreviation |
ASPRO |
| Alternative Names |
N/A |
| Range |
Request Information |
| Sensitivity |
Request Information |
| Sample Type |
Serum, Plasma, Other biological fluids |
| Detection Method |
Sandwich |
| Analysis Method |
Quantitive |
| Assay Duration |
1-4.5h |
| Sample Volume |
1-200 μL |
| Detection Wavelengt |
450 nm |
Test principle
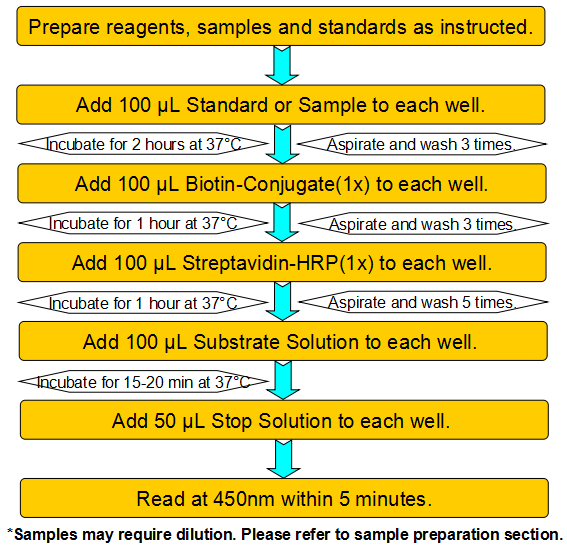
This assay employs a two-site sandwich ELISA to quantitate ASPRO in samples. An antibody specific for ASPRO has been pre-coated onto a microplate. Standards and samples are pipetted into the wells and any ASPRO present is bound by the immobilized antibody. After removing any unbound substances, a biotin-conjugated antibody specific for ASPRO is added to the wells. After washing, Streptavidin conjugated Horseradish Peroxidase (HRP) is added to the wells. Following a wash to remove any unbound avidin-enzyme reagent, a substrate solution is added to the wells and color develops in proportion to the amount of ASPRO bound in the initial step. The color development is stopped and the intensity of the color is measured.
Product Overview
Asprosin is a protein hormone produced by mammals in their fatty (white adipose) tissues that stimulates the liver to release glucose into the blood stream. Asprosin is secreted by white adipose, circulates at nanomolar levels, and is recruited to the liver, where it activates the G protein-cAMP-PKA pathway, resulting in rapid glucose release into the circulation. Humans and mice with insulin resistance show pathologically elevated plasma asprosin, and its loss of function via immunologic or genetic means has a profound glucose- and insulin-lowering effect secondary to reduced hepatic glucose release. Asprosin represents a glucogenic protein hormone, and therapeutically targeting it may be beneficial in type II diabetes and metabolic syndrome.
Components
Reagents |
Quantity |
Reagents |
Quantity |
Assay plate (96 Wells) |
1 |
Instruction manual |
1 |
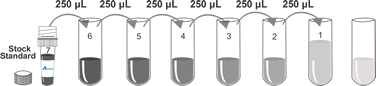
Standard (lyophilized) |
2 |
Sample Diluent |
1 x 20 mL |
Biotin-Conjugate (concentrate 100 x) |
1 x 120 μL |
Biotin-Conjugate Diluent |
1 x 12 mL |
Streptavidin-HRP (concentrate 100 x) |
1 x 120 μL |
Streptavidin-HRP Diluent |
1 x 12 mL |
Wash Buffer (concentrate 25 x) |
1 x 20 mL |
Substrate Solution |
1 x 10 mL |
Stop Solution |
1 x 6 mL |
Adhesive Films |
4 |
Specificity
This assay has high sensitivity and excellent specificity for detection of Human ASPRO. No significant cross-reactivity or interference between Human ASPRO and analogues was observed.
Recovery
Matrices listed below were spiked with certain level of recombinant Human ASPRO and the recovery rates were calculated by comparing the measured value to the expected amount of Human ASPRO in samples.
Precision
Intra-assay Precision (Precision within an assay) Three samples of known concentration were tested twenty times on one plate to assess intra-assay precision. Inter-assay Precision (Precision between assays) Three samples of known concentration were tested in forty separate assays to assess inter-assay precision. CV (%) = SD/meanX100 Intra-Assay: CV<8% Inter-Assay: CV<12%
Linearity
The linearity of the kit was assayed by testing samples spiked with appropriate concentration of Human ASPRO and their serial dilutions. The results were demonstrated by the percentage of calculated concentration to the expected.
Stability
The stability of ELISA kit is determined by the loss rate of activity. The loss rate of this kit is less than 5% within the expiration date under appropriate storage condition. The loss rate was determined by accelerated thermal degradation test. Keep the kit at 37°C for 4 and 7 days, and compare O.D.values of the kit kept at 37°C with that of at recommended temperature. (referring from China Biological Products Standard, which was calculated by the Arrhenius equation. For ELISA kit, 4 days storage at 37°C can be considered as 6 months at 2 - 8°C, which means 7 days at 37°C equaling 12 months at 2 - 8°C).
Sample collection and storage
Serum: Use a serum separator tube (SST) and allow samples to clot for two hours at room temperature or overnight at 2 - 8°C before centrifugation for 15 minutes at 1000 × g. Remove serum and assay immediately or aliquot and store samples at ≤ -20°C. Avoid repeated freeze-thaw cycles. Plasma: Collect plasma using EDTA, or heparin as an anticoagulant. Centrifuge for 15 minutes at 1000 × g at 2 - 8°C within 30 minutes of collection. Assay immediately or aliquot and store samples at ≤ -20°C. Avoid repeated freeze-thaw cycles. Other biological fluids: Centrifuge samples for 20 minutes at 1000 × g. Remove particulates and assay immediately or store samples in aliquot at -20°C or -80°C. Avoid repeated freeze/thaw cycles.
Kits storage instructions
Store at 2-8°C. Please refer to Instruction Manual.




 Phone:
Phone:  E-mail:
E-mail:  Address:
Address: